Hip pain in women: causes, symptoms and effective treatment options

A woman holding her hip in pain.
Hip pain ranks among the most frequent complaints I see from women at my clinic. It affects women across every age group, from young athletes dealing with labral tears to postmenopausal women struggling with osteoarthritis. The pain can make simple tasks like walking to the kitchen, climbing a flight of stairs, or even turning over in bed feel like a challenge.
What makes hip pain particularly common in women isn't coincidence. It's anatomy, hormones, and biomechanics working together. Women have wider pelvises, experience hormonal fluctuations throughout life, and undergo pregnancy-related changes that directly affect joint stability. Understanding these causes, and knowing when to seek help — can prevent months or years of unnecessary suffering.
Understanding Hip pain in women
The hip is a ball-and-socket joint, one of the largest weight-bearing joints in the body. The femoral head (ball) fits into the acetabulum (socket) of the pelvis, and together they support nearly every lower body movement, walking, bending, squatting, rotating, sitting down, standing up.
In women, the pelvis is naturally wider and more shallow to accommodate childbirth. This anatomical difference changes the angle at which the femur meets the pelvis (known as the Q-angle), and it shifts the load distribution across the hip joint. Over time, this can increase susceptibility to cartilage wear, muscle strain, and bursitis. It's not a design flaw, it's a biomechanical trade-off, and it explains why hip problems show up earlier and more frequently in women.
Why Hip pain Is more common in women
Several biological and lifestyle factors make women more vulnerable to hip pain than men.
Hormonal changes
Estrogen does more than regulate reproductive function. It protects cartilage, maintains bone density, and supports ligament elasticity. During the menstrual cycle, estrogen levels fluctuate — and some women report increased joint laxity and discomfort during the luteal phase.
The most dramatic shift happens at menopause. When estrogen drops significantly, cartilage degradation accelerates, bone density decreases (osteoporosis risk increases by 20-30% in the first 5-7 years post-menopause), and the protective cushioning within the hip joint starts thinning. This is precisely why osteoarthritis rates spike in women after age 50.
Wider pelvis and altered biomechanics
A wider pelvis creates a larger Q-angle between the hip and knee. This angle increases lateral stress on the hip abductor muscles, the iliotibial band, and the trochanteric bursa. Women who run, walk long distances, or stand for extended periods often develop pain along the outer hip, a direct result of this biomechanical setup.
Pregnancy and postpartum changes
During pregnancy, the body releases relaxin, a hormone that loosens pelvic ligaments to prepare for delivery. While necessary, relaxin doesn't target only the pelvis. It affects ligaments throughout the body, making all joints (including the hips) temporarily less stable.
The added weight of pregnancy (typically 10-15 kg) further loads the hip joint. Many women develop sacroiliac joint dysfunction, symphysis pubis dysfunction, or hip bursitis during the third trimester. Some of these problems persist postpartum, especially if core and pelvic floor rehabilitation isn't prioritized.
Weak gluteal and core muscles
Desk-bound lifestyles weaken the gluteus medius — a muscle critical for hip stability. When this muscle can't do its job, the hip joint compensates by absorbing more impact during walking and standing. I've seen this pattern repeatedly in women aged 25-45 who sit 8-10 hours daily. The hip pain they experience isn't from arthritis, it's from muscular imbalance.
Common causes of Hip pain in women
Osteoarthritis
The most common cause of chronic hip pain in women over 40. Cartilage, the smooth tissue that cushions the joint — gradually wears down, leaving bone rubbing against bone. Symptoms include deep groin pain, stiffness after sitting, reduced range of motion, and pain that worsens with activity. X-rays typically show joint space narrowing, osteophyte formation, and subchondral sclerosis.
Trochanteric bursitis
The trochanteric bursa sits on the outer bony prominence of the hip. When inflamed, it produces sharp, burning pain on the outer hip that worsens when lying on the affected side, climbing stairs, or crossing legs. It's 3-4 times more common in women than men. Diagnosis is clinical, tenderness on direct palpation over the greater trochanter is the hallmark sign.
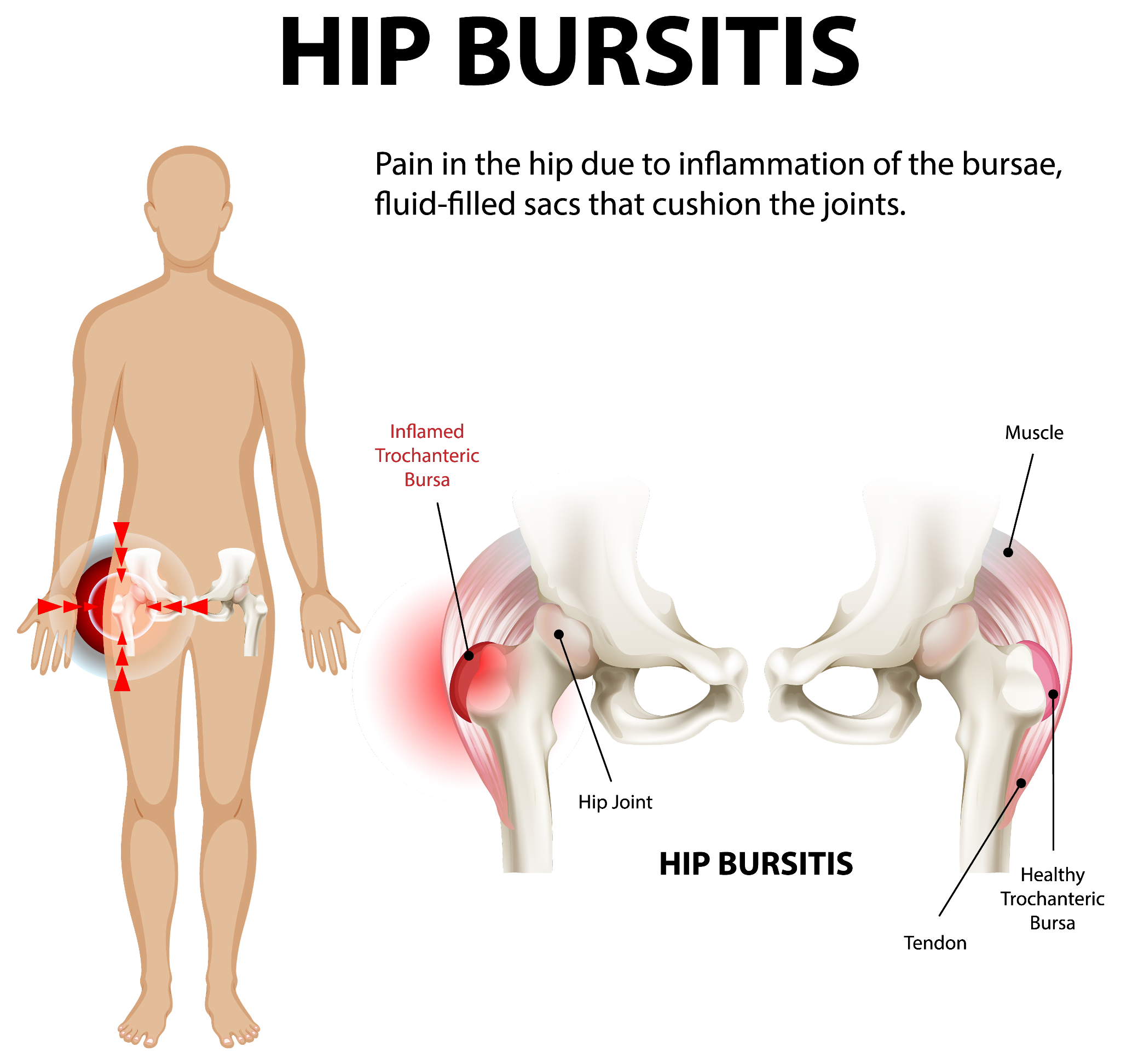
An infographic illustrating hip bursitis.
Hip labral tear
The labrum is a ring of fibrocartilage that deepens the hip socket and stabilizes the joint. Tears can result from sports (especially those involving twisting, like tennis or dance), repetitive hip flexion, or structural abnormalities like hip dysplasia or femoroacetabular impingement (FAI). Symptoms include a deep ache or catching sensation in the groin, clicking during movement, and pain that worsens with prolonged sitting or pivoting.
MRI arthrogram is the gold standard for diagnosis. Not every labral tear needs surgery — many respond well to physiotherapy and activity modification.
Sciatica
Sciatic nerve compression can produce pain that starts in the lower back or buttock and radiates down through the hip and leg. Women who sit for long hours, have poor lumbar posture, or are in their third trimester of pregnancy are at higher risk. The pain is typically one-sided and may come with tingling, numbness, or weakness in the leg.
Tendinitis
Inflammation of the hip tendons, particularly the iliopsoas tendon (the primary hip flexor), causes pain in the front of the hip that worsens with stair climbing, running, or bringing the knee toward the chest. It's common in runners and women who do high-intensity interval training without adequate warm-up.
Pelvic joint dysfunction (Sacroiliac joint)
The sacroiliac (SI) joint connects the spine to the pelvis. Dysfunction here — from pregnancy, a fall, or chronic postural imbalance, produces pain in the lower back and buttock that can mimic hip pain. A focused physical examination with provocative tests (FABER, Gaenslen's, compression test) helps differentiate SI joint pain from true hip pathology.
Hip fractures
Postmenopausal women with osteoporosis face a significantly elevated fracture risk. A hip fracture can occur from a simple fall, even from standing height. This is a medical emergency requiring urgent surgical fixation, typically within 24-48 hours to reduce complications.
When Hip pain requires immediate medical help
See an orthopedic specialist without delay if you experience:
- Sudden, severe hip pain — especially after a fall
- Inability to bear weight or walk
- Visible deformity or swelling around the hip
- Redness, warmth, or fever with joint pain (could indicate infection)
- Pain persisting beyond 2-3 weeks despite rest and home care
- Night pain that consistently wakes you from sleep
- Numbness, tingling, or weakness radiating down the leg
- Progressive loss of hip range of motion
Ignoring persistent hip pain doesn't just mean living with discomfort. Untreated hip conditions can lead to compensatory problems in the knee, lower back, and opposite hip.
What You Can Do to reduce Hip pain
Strengthen the Hip and core muscles
Muscle weakness is the single most correctable cause of hip pain in women under 50. A targeted strengthening program can reduce pain by 40-60% within 6-8 weeks for conditions like bursitis and tendinitis.
Effective exercises include:
- Glute bridges, 3 sets of 12-15 reps, focusing on squeezing at the top
- Side-lying leg raises, targets the gluteus medius directly
- Clamshells with resistance band — builds hip external rotator strength
- Wall squats, controlled loading without excessive joint stress
- Dead bugs and planks, core stability that takes pressure off the hip
Start without weights. Progress gradually. If an exercise increases pain, stop and reassess with your physiotherapist.
Apply heat or Ice strategically
Ice works best for acute flare-ups — bursitis pain after a long walk, for example. Apply for 15 minutes with a cloth barrier to prevent skin burns. Heat (a warm towel or heating pad) is better for chronic stiffness and muscle tightness. Apply for 15-20 minutes before stretching or exercise.
Maintain a healthy body weight
Every kilogram of excess body weight translates to roughly 3-4 kg of additional force across the hip joint during walking. Losing even 5 kg can meaningfully reduce hip joint loading and slow cartilage wear in early osteoarthritis.
Fix your posture
Slouching compresses the hip flexors and tilts the pelvis forward (anterior pelvic tilt), increasing strain on the hip joint. If you work at a desk, use a chair that supports your lumbar curve. Stand up and walk for 2-3 minutes every 30-40 minutes. Avoid crossing your legs, it rotates the pelvis and loads the hip asymmetrically.
Choose supportive footwear
High heels shift your center of gravity forward, increasing hip flexor strain and lumbar lordosis. Flat shoes without arch support aren't much better, they allow the foot to pronate excessively, which rotates the tibia and loads the hip joint unevenly. Look for shoes with moderate arch support, cushioned soles, and a heel drop of no more than 2-3 cm.
Adjust your sleeping position
If one hip is painful, avoid sleeping on that side. Place a firm pillow between your knees when sleeping on the opposite side — this keeps the pelvis aligned and reduces tension on the hip muscles. A mattress that's too soft lets the hip sink in and creates awkward angles. Medium-firm mattresses generally work best for hip pain.
Include bone-Healthy nutrition
Calcium (1000-1200 mg daily for women over 50), vitamin D (800-1000 IU daily), protein, and omega-3 fatty acids all support bone density and joint health. Dairy, leafy greens, fatty fish, nuts, and seeds should be regular parts of your diet. For postmenopausal women, a DEXA scan every 2 years helps monitor bone density and guide supplementation.
Physiotherapy
A physiotherapist trained in hip rehabilitation can identify the exact muscles that need strengthening, the movement patterns that need correction, and the stretches that'll help most. Physiotherapy isn't a one-size-fits-all prescription, it should be tailored to your specific diagnosis.

A woman undergoing physiotherapy for pain relief.
Medications and medical treatment
Treatment depends entirely on the diagnosis. For bursitis and tendinitis, a short course of NSAIDs (anti-inflammatory medications) combined with physiotherapy often resolves the problem within 4-6 weeks. Corticosteroid injections into the trochanteric bursa can provide rapid relief for stubborn cases, though they're typically limited to 2-3 injections per year.
For osteoarthritis, treatment ranges from activity modification and weight management in early stages to viscosupplementation (hyaluronic acid injections) in moderate cases. When cartilage loss is severe and conservative measures fail, hip replacement surgery becomes the most reliable option, with modern implants lasting 20-25 years in most patients.
For labral tears, treatment depends on severity. Small tears with minimal symptoms respond to physiotherapy and activity modification. Larger tears causing mechanical symptoms (clicking, locking, giving way) may require arthroscopic surgery.
Early diagnosis consistently leads to better outcomes. The longer hip pain goes untreated, the more compensatory patterns develop — and those secondary problems become their own source of pain.
If you're dealing with persistent hip pain, expert evaluation makes a measurable difference. Dr. Ankur Singh provides advanced orthopedic care backed by international training and years of clinical experience. His patient-focused approach ensures accurate diagnosis and effective treatment for conditions like hip arthritis, bursitis, fractures, and chronic pain.
The bottom line
Hip pain in women isn't something to accept as normal. It has specific, identifiable causes, and most of them are treatable. Whether the problem is muscular weakness, hormonal changes, bursitis, or early arthritis, the right combination of diagnosis, targeted exercise, lifestyle modification, and medical treatment can restore comfort and mobility. Waiting and hoping the pain goes away on its own usually means the underlying condition progresses further. Get assessed early. Treat it properly. Stay active.
Medical Disclaimer
The information provided on this website is for educational purposes only and should not be considered as medical advice. Please consult Dr. Ankur Singh or a qualified healthcare professional for personalized medical guidance.






























