ACL Injuries: Why They are Increasing & How to Avoid Them
=========================================================

Athlete suffering ACL injury during sudden knee twist.
ACL tears have become one of the most common knee injuries I treat at my clinic in Noida. And it's not just professional athletes walking in with this problem, I'm seeing weekend cricketers, college football players, gym-goers who landed wrong during a box jump, and even middle-aged patients who twisted their knee stepping off a curb. The ACL (Anterior Cruciate Ligament) is one of four major ligaments holding your knee together, and when it tears, you know it immediately. There's usually a "pop," the knee swells within hours, and putting weight on that leg feels deeply unstable.
What concerns me most is the trend. ACL injuries are rising, especially among younger populations and women. Understanding why this is happening, and what you can actually do about it — matters far more than most people realize.
What is an ACL Injury?
The ACL connects your femur (thighbone) to your tibia (shinbone). It sits deep inside the knee joint and prevents the tibia from sliding forward relative to the femur. It also provides rotational stability, which is why sports involving pivoting, cutting, and sudden direction changes put tremendous stress on this ligament.
An ACL injury can range from a mild stretch (Grade 1 sprain) to a complete rupture (Grade 3). Most of the injuries I see clinically are Grade 2 or Grade 3, partial or complete tears.
Common symptoms include:
- A sudden "pop" sound or sensation at the moment of injury
- Severe knee pain that makes it hard to continue any activity
- Rapid swelling — typically within the first 2-6 hours
- Feeling like the knee is "giving way" or buckling when you try to stand
- Difficulty walking or bearing weight
- Loss of full range of motion, particularly full extension
One thing many patients don't realize: an ACL tear doesn't always cause constant pain after the initial episode. The swelling goes down, the acute pain fades, and people assume it's healed. It hasn't. The instability remains, and without proper treatment, every time you pivot or twist, you risk damaging the meniscus and cartilage, creating problems that are much harder to fix.
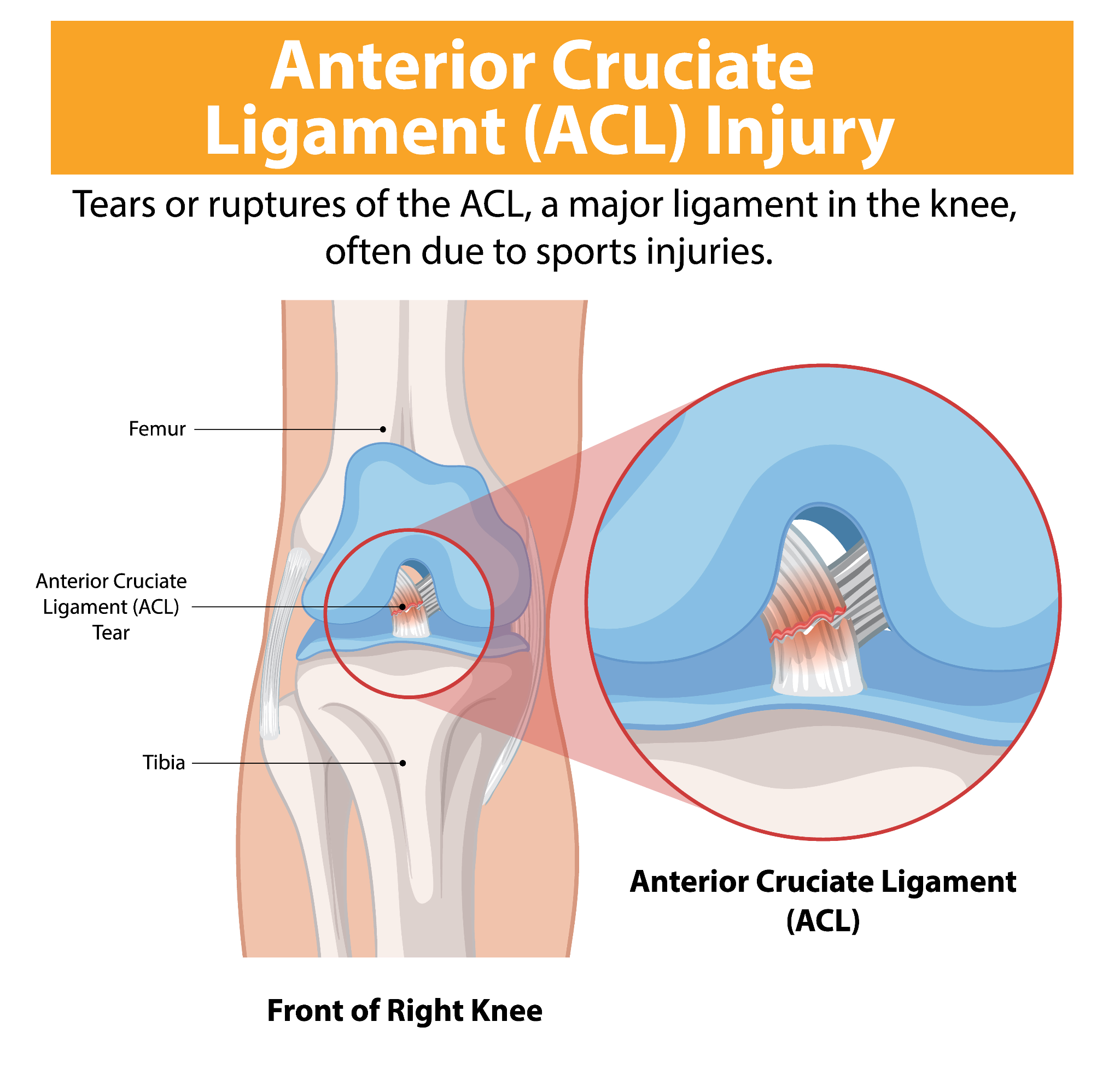
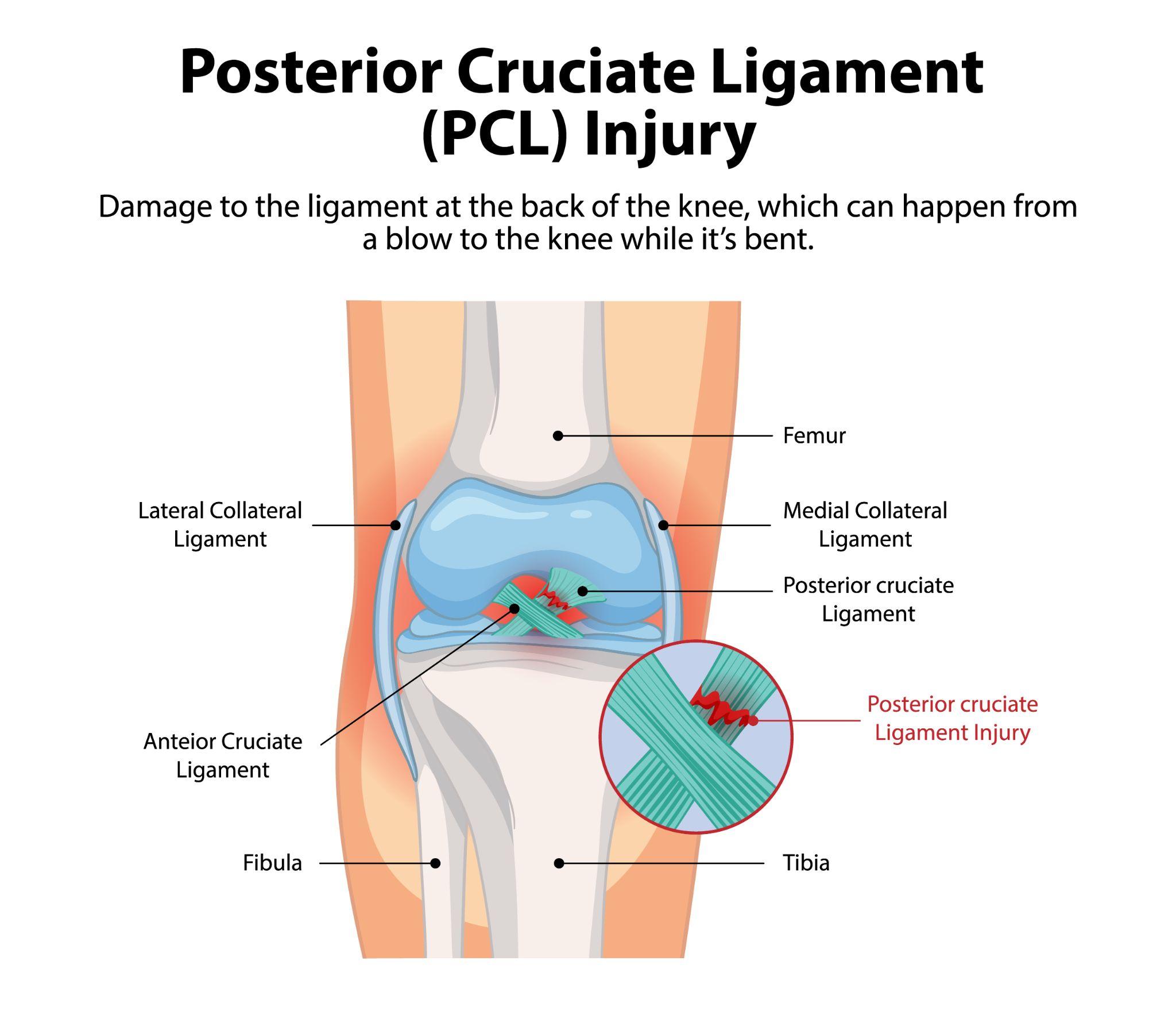
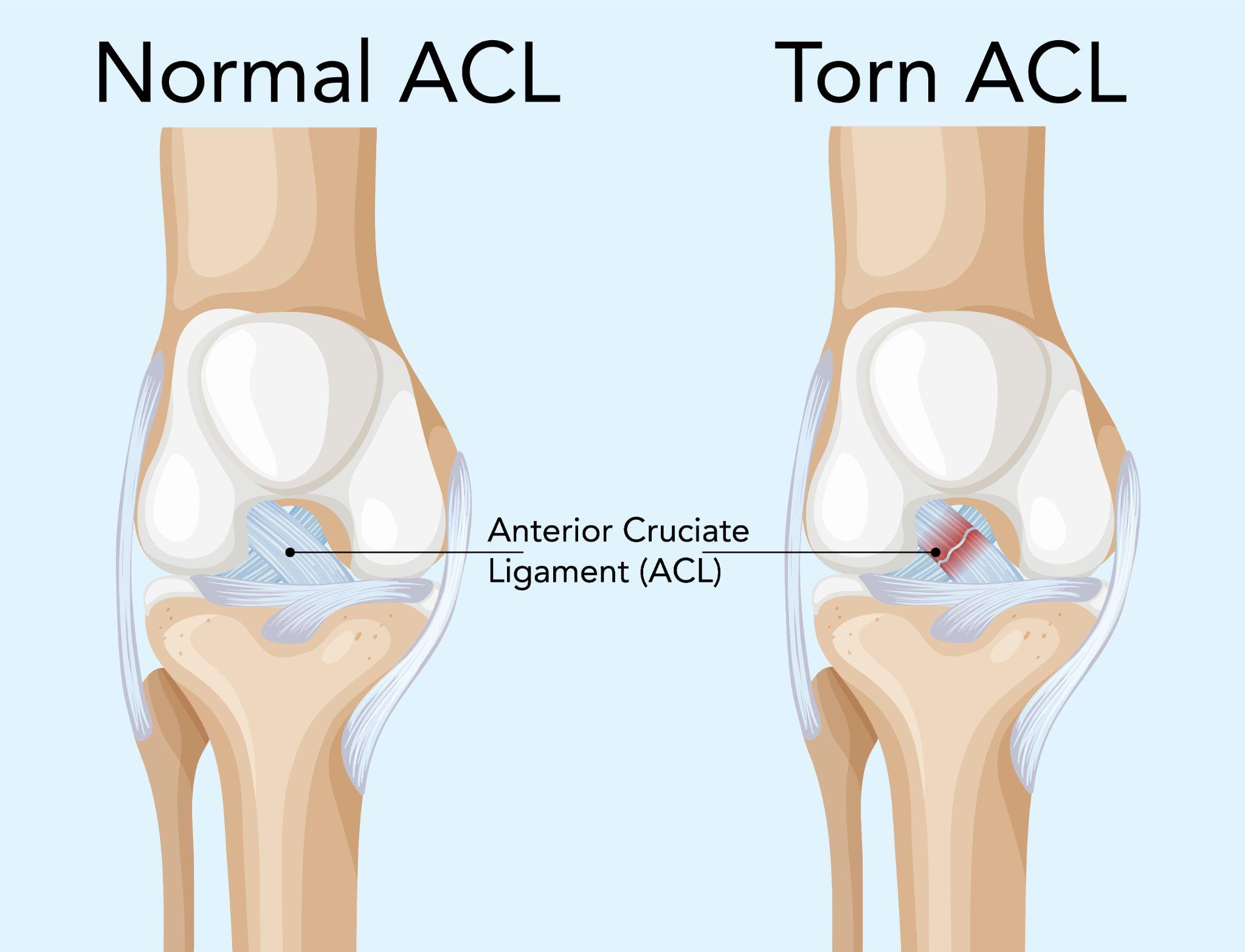
Medical infographic explaining ACL tear in the knee joint.
Why Are ACL Injuries on the Rise?
This isn't just perception, the data backs it up. ACL injury rates have increased measurably over the past two decades, particularly among adolescents and young adults. Several factors are driving this.
1. increased sports participation
More people are playing high-intensity sports — football, basketball, soccer, badminton, kabaddi, than ever before. That includes younger children starting competitive sports at 8-10 years old, often without any formal training in movement mechanics. More exposure to cutting, pivoting, and jumping movements means more ACL injuries. The math is straightforward.
2. early specialization in sport
When a child plays only cricket 12 months a year, or only football, the same movement patterns get repeated thousands of times. This creates muscle imbalances and overloads specific structures, including the ACL. Varied sports participation builds more balanced strength and coordination. Single-sport athletes lose that protective diversity.
3. higher intensity training
The athletic demands have gone up significantly. Training sessions are longer, more intense, and more frequent. Recovery periods are shorter. When muscles fatigue, they stop absorbing shock effectively. That shock transfers directly to the ligaments.
4. biomechanical differences in women
This is a clinical reality we see clearly in the numbers. Women sustain ACL injuries at 2-8 times the rate of men in the same sports. Several anatomical and hormonal factors contribute:
- A wider pelvis creates a larger Q-angle at the knee, increasing inward stress
- The intercondylar notch (the groove where the ACL sits) tends to be narrower in women
- Hormonal fluctuations — particularly estrogen, affect ligament laxity throughout the menstrual cycle
- Women tend to land with less knee flexion and more valgus (knock-knee) positioning
These aren't things you can change, but they are things you can train around with proper neuromuscular conditioning.
5. improper footwear & playing surfaces
I've treated injuries that trace back directly to worn-out shoes on artificial turf. High-grip surfaces combined with cleats create a "foot lock" situation, the foot stays planted while the body rotates, and the ACL takes the entire torsional force. Concrete courts, uneven ground, and shoes without proper ankle support all add to the risk.
Risk Factors for ACL Injuries
Some people are more vulnerable than others. Being aware of these risk factors helps with targeted prevention:
- Previous knee injury: If you've torn one ACL, you're 3-6 times more likely to tear the other one. The rebuilt knee is strong, but the opposite knee often compensates and takes on abnormal loading patterns.
- Weak hamstrings and glutes: The hamstrings work as a dynamic stabilizer for the ACL. When they're weak relative to the quadriceps (a ratio below 0.6), the ACL bears significantly more stress during deceleration.
- Poor landing mechanics: Landing with straight knees, knees caving inward, or on one leg without control — these are patterns I see repeatedly in patients who've torn their ACL.
- Sudden return to sport after a break: This is extremely common. Someone hasn't played for months, jumps into a competitive match at full intensity, and the body isn't prepared. Muscle conditioning drops faster than most people expect.
- Fatigue: Most ACL tears don't happen in the first quarter. They happen late in the game, late in the practice session, when muscles are tired and reaction times are slower.
- Age and gender: Highest risk between ages 15-25, with females at significantly elevated risk.
How to Prevent ACL Injuries
Prevention isn't about avoiding sports. It's about preparing the body properly. Research consistently shows that structured neuromuscular training programs can reduce ACL injury risk by 50-70%. That's a substantial reduction for relatively simple interventions.
1. strengthen the right muscles
The quadriceps, hamstrings, glutes, and core all need to be strong, but more than that, they need to be balanced. I specifically recommend:
- Squats and lunges with proper form (knee tracking over the toe, not caving inward)
- Romanian deadlifts and hamstring curls to build posterior chain strength
- Single-leg exercises like Bulgarian split squats and step-ups, these expose and correct side-to-side imbalances
- Hip abductor and glute medius work to prevent knee valgus
2. improve flexibility & balance
Tight muscles limit joint range of motion and create compensatory movement patterns. A consistent stretching routine targeting the hamstrings, hip flexors, quads, and calves keeps the muscles around the knee supple. Balance training — single-leg stands, wobble boards, BOSU ball exercises, trains the proprioceptive system that provides real-time stability to the knee.
3. learn proper movement techniques
This is the single most impactful prevention strategy. Athletes need to be taught how to:
- Land from jumps with knees bent at roughly 30 degrees, not locked straight
- Decelerate using a three-step pattern rather than a sudden plant-and-stop
- Cut and pivot with the knee aligned over the foot, avoiding inward collapse
- Absorb force through the hips and glutes, not the knees alone
Coaches and physiotherapists should drill these patterns until they become automatic. Conscious technique breaks down under game pressure, only ingrained muscle memory holds up.
4. Use of protective gear & footwear
Sport-specific shoes with appropriate traction for the playing surface matter. Replace shoes when the treads wear down — most athletic shoes need replacement every 6-8 months of regular use. For individuals with a history of ACL injury, a functional knee brace during sports can provide an additional layer of confidence and mild mechanical support, though it's not a substitute for proper conditioning.
5. avoid overtraining
Rest days aren't laziness, they're when your body actually repairs and strengthens. Tendons and ligaments, unlike muscles, have poor blood supply and recover slowly. Consecutive high-intensity sessions without adequate rest create cumulative micro-damage that eventually leads to a macro-injury.
Cross-training between different activities, swimming one day, running another, strength work in between — reduces repetitive stress on any single joint.
6. neuromuscular training programs
Programs like the FIFA 11+ (designed for football but adaptable) have strong evidence behind them. These 15-20 minute warm-up routines combine:
- Dynamic stretching
- Plyometric exercises (controlled jumping and landing)
- Balance and proprioception drills
- Core stability work
- Sport-specific agility patterns
Teams that implement these programs consistently see dramatic reductions in ACL injuries. The key word is consistently, doing it once a week doesn't work. It needs to be part of every training session warm-up.
When to See a Doctor
If you experience any of the following, get evaluated by an orthopedic surgeon, don't wait:
- A "pop" in the knee during activity
- Rapid swelling within hours of an injury
- Knee instability — feeling like it might give way when you walk or stand
- Inability to bear weight on the injured leg
- Pain that persists beyond 48 hours with rest and ice
- The knee locking or catching during movement
An MRI is typically needed to confirm the diagnosis and assess whether the meniscus or other structures are also damaged. I also perform specific clinical tests, the Lachman test, anterior drawer test, and pivot shift test, during the physical examination. These are quite reliable in experienced hands and often point to the diagnosis before the MRI is even done.
Delaying evaluation is a mistake I see too often. Patients walk around on an ACL-deficient knee for weeks or months, and by the time they come in, there's additional meniscal damage that wasn't there initially. That meniscal tear then complicates the surgery and extends the rehabilitation.

Orthopedic doctor examining knee of patient with ACL injury.
Treatment Options
The right treatment depends on your injury severity, age, activity level, and what you want to get back to doing. There's no one-size-fits-all answer.
1. non-Surgical
Non-surgical management can work for partial ACL tears in patients who don't play pivoting sports and are willing to modify their activity level. This involves:
- Structured physiotherapy focusing on quadriceps and hamstring strengthening
- Proprioceptive and balance training to compensate for the lost ligament stability
- Use of a functional brace during physical activity
- Activity modification — avoiding cutting, pivoting, and high-impact sports
For older patients or those with lower physical demands, this approach can provide a functional, stable knee for daily activities. But I'll be honest, for young, active individuals who want to return to competitive sports, non-surgical management has a high rate of re-injury and secondary damage.
2. surgical (ACL reconstruction)
ACL reconstruction is the standard surgical treatment. The torn ligament cannot be stitched back together, it needs to be replaced with a graft. Common graft options include:
- Hamstring tendon autograft: Taken from the patient's own hamstring tendons. Less anterior knee pain, but slightly slower hamstring recovery.
- Patellar tendon autograft (bone-tendon-bone): Considered the gold standard by many surgeons. Strong fixation, reliable healing, but can cause anterior knee pain.
- Quadriceps tendon autograft: Gaining popularity, good strength, less donor site morbidity.
- Allograft (donor tissue): Used in revision cases or multi-ligament injuries. Avoids donor site issues but has a slightly higher re-rupture rate in young athletes.
The surgery itself is arthroscopic — performed through 2-3 small incisions with a camera and specialized instruments. Most patients go home the same day.
Recovery and Rehabilitation
Rehabilitation after ACL reconstruction is where the real work happens. Surgery gives you a new ligament. Rehab gives you a functional knee. Cutting corners here is the fastest way to a poor outcome or re-tear.
Phase 1 (Weeks 0-2): Reduce swelling, protect the graft, regain full knee extension. Weight-bearing with crutches as tolerated. Gentle quad activation exercises.
Phase 2 (Weeks 2-6): Progressive weight-bearing, stationary cycling, closed-chain strengthening (leg press, mini-squats). The focus is on quad and hamstring activation without stressing the healing graft.
Phase 3 (Months 2-4): Full weight-bearing, progressive strengthening with increasing resistance. Single-leg balance work, proprioception training, swimming and cycling for cardiovascular fitness.
Phase 4 (Months 4-6): Sport-specific agility drills, lateral movements, controlled jumping and landing. Gradual progression toward full-speed activities.
Return to Sport (Months 9-12): Most surgeons recommend waiting at least 9 months before returning to competitive, pivoting sports. Return-to-sport testing, including strength testing, hop tests, and movement quality assessment, should confirm readiness. Returning too early is the single biggest risk factor for re-tearing the graft.
The full rehabilitation process takes commitment. Patients who follow their rehab program diligently return to their pre-injury level of activity in the vast majority of cases.
Dietary and recovery tips
Proper nutrition supports ligament healing and tissue repair during the recovery period:
- Protein: Adequate protein intake (1.2-1.6g per kg body weight) supports collagen synthesis and muscle recovery. Eggs, chicken, paneer, dal, fish — spread protein intake across all meals.
- Vitamin C: Directly involved in collagen formation. Citrus fruits, amla, bell peppers, guava.
- Calcium and Vitamin D: Bone health supports joint health. If your Vitamin D levels are low (extremely common in Indian patients), get them corrected with supplementation.
- Anti-inflammatory foods: Turmeric, ginger, omega-3 fatty acids (walnuts, flaxseed, fatty fish) can help manage inflammation during recovery.
- Hydration: Tendons and cartilage depend on proper hydration to maintain elasticity.
Avoid smoking and excessive alcohol during recovery, both impair tissue healing significantly.
Expert ACL Care at Dr. Ankur Singh's Clinic, Noida
At KDSG Superspeciality Hospitals, Noida, I treat ACL injuries using current, evidence-based protocols. My approach includes:
- Thorough clinical examination combined with advanced imaging (MRI, dynamic ultrasound) for precise diagnosis
- Individualized treatment planning, I don't recommend surgery to every ACL patient. Some do well with structured rehabilitation alone.
- Arthroscopic ACL reconstruction using carefully selected graft options based on the patient's age, activity level, and anatomy
- Structured, phased rehabilitation programs with clear milestones and return-to-sport criteria
- Injury prevention guidance for athletes — including pre-season screening and movement analysis
Having trained internationally and treated hundreds of ACL cases, I understand that this injury is more than a physical problem. It affects confidence, livelihood for athletes, and daily quality of life. A transparent, patient-specific approach gets the best results.
Final Thoughts
ACL injuries are increasing, but they're also highly preventable. Proper neuromuscular training, balanced strength conditioning, sport-specific movement coaching, and adequate rest can cut your risk dramatically. For young athletes, and particularly for young women in sports, structured prevention programs should be as routine as practice itself.
If an injury does happen, early diagnosis and appropriate treatment make all the difference. A well-performed ACL reconstruction followed by disciplined rehabilitation allows most patients to return to full activity, including competitive sports.
Your knees carry you through every step, every sprint, every pivot on the field. Take care of them with smart training, proper recovery, and professional guidance when something goes wrong.
Medical Disclaimer
The information provided on this website is for educational purposes only and should not be considered as medical advice. Please consult Dr. Ankur Singh or a qualified healthcare professional for personalized medical guidance.