Shoulder Pain: Common Reasons, Diagnosis, and Treatment Options
===============================================================

A close-up image showing shoulder discomfort commonly associated with rotator cuff pain or shoulder injury.
The shoulder is the most mobile joint in the human body, and that exceptional range of motion comes at a cost. Unlike the hip, which sits in a deep bony socket, the shoulder's socket (glenoid) is remarkably shallow. This design allows you to reach overhead, throw a ball, and rotate your arm in nearly every direction, but it also makes the shoulder inherently vulnerable to injury and wear.
Shoulder pain is something I evaluate daily at my practice. Patients come in unable to comb their hair, hook a bra strap, lift a bag of groceries, or sleep on their side. Some have been dealing with it for weeks; others for months. The cause can range from a simple muscle strain that settles in a few days to a full-thickness rotator cuff tear that requires surgical repair. Getting the diagnosis right early is what separates a quick recovery from a prolonged one.
Anatomy of the shoulder joint
Understanding a bit of shoulder anatomy helps make sense of why certain injuries cause specific symptoms.
The shoulder is a ball-and-socket joint formed by the head of the humerus (upper arm bone) sitting against the glenoid cavity of the scapula (shoulder blade). The socket is deepened slightly by a ring of cartilage called the labrum. Surrounding this joint are four muscles and their tendons, collectively called the rotator cuff:
- Supraspinatus — initiates arm abduction (lifting the arm away from the body). This is the most commonly torn rotator cuff tendon
- Infraspinatus, externally rotates the arm
- Teres minor, assists with external rotation
- Subscapularis — the only rotator cuff muscle on the front of the shoulder; it internally rotates the arm
Above the rotator cuff lies a fluid-filled sac called the subacromial bursa, which cushions the tendons as they glide beneath the acromion (the bony projection at the top of the shoulder blade). When this space narrows, from bone spurs, swelling, or poor posture, the tendons and bursa get pinched, producing pain with overhead movements.
The shoulder also relies on ligaments and the joint capsule for stability, and larger muscles like the deltoid, pectoralis major, and trapezius for power and coordinated movement.
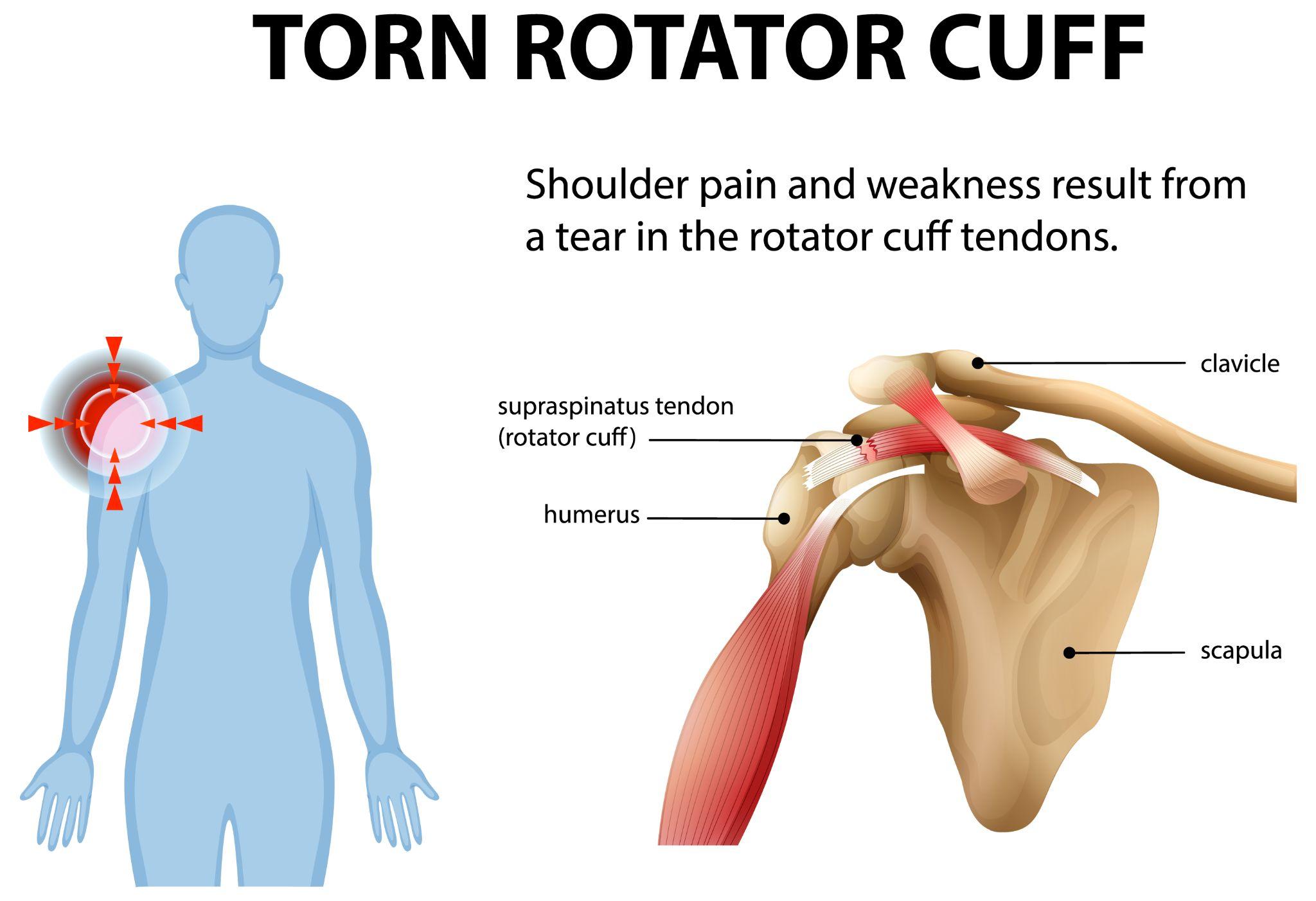
Diagram showing a rotator cuff tear as a common cause of shoulder pain and weakness.
Common shoulder pain causes
Rotator cuff injuries
This is the most frequent diagnosis I make in patients with shoulder pain over the age of 40. Rotator cuff problems exist on a spectrum:
- Tendinitis — inflammation of the tendon, usually the supraspinatus, from overuse or repetitive overhead activity. Common in painters, carpenters, and recreational athletes who play badminton or tennis
- Partial tear, some fibers of the tendon are damaged but the tendon is still intact. Produces pain with specific movements, especially reaching overhead or behind the back
- Full-thickness tear, the tendon is torn completely through. Causes significant weakness — patients often can't lift their arm above shoulder level, or they feel it "give way" under load
Rotator cuff tears can result from acute injuries (a fall on an outstretched hand, lifting something too heavy) or from gradual degeneration. After age 50, degenerative tears become increasingly common even in people who haven't had a specific injury. Not every tear requires surgery, many partial tears and even some full-thickness tears in older adults respond well to physiotherapy.
Frozen shoulder (Adhesive capsulitis)
Frozen shoulder is a condition where the joint capsule thickens and tightens, severely restricting movement. It progresses through three stages:
- Freezing stage (6 weeks to 9 months), pain increases gradually, and range of motion starts to decrease
- Frozen stage (4 to 12 months) — pain may decrease slightly, but stiffness is at its worst. Patients struggle to raise the arm, reach behind the back, or rotate the shoulder outward
- Thawing stage (6 to 24 months), motion gradually returns
Frozen shoulder affects about 2–5% of the general population, but the rate jumps to 10–20% among diabetic patients. It's also more common after prolonged immobilization (e.g., after a fracture or surgery), in thyroid disorder patients, and more frequently in women than men.
The total duration of frozen shoulder can stretch from 1 to 3 years if left untreated. Guided physiotherapy, steroid injections, and in some cases, manipulation under anesthesia or arthroscopic capsular release can significantly shorten the timeline.
Shoulder arthritis
Osteoarthritis of the shoulder involves progressive loss of cartilage in the glenohumeral joint. The smooth cartilage surface wears down, exposing bone, causing pain, stiffness, and a grinding or crunching sensation (crepitus) with movement.
Primary shoulder arthritis is more common after age 60. Secondary arthritis can develop earlier in patients with a history of shoulder fractures, recurrent dislocations, rotator cuff tears, or inflammatory conditions like rheumatoid arthritis.
Symptoms typically worsen over years. Early stages respond to activity modification, NSAIDs, physiotherapy, and occasional corticosteroid injections. Advanced arthritis with bone-on-bone contact and significant functional limitation may require shoulder replacement surgery (total shoulder arthroplasty or reverse shoulder arthroplasty).
Shoulder impingement syndrome
Impingement occurs when the supraspinatus tendon and subacromial bursa are compressed in the narrow space beneath the acromion during arm elevation. The resulting inflammation produces pain, typically a sharp catch when raising the arm between 60 and 120 degrees (the "painful arc").
Risk factors include poor posture (rounded shoulders, forward head), weak rotator cuff muscles, overhead work, and bone spurs on the underside of the acromion. Impingement is often the precursor to rotator cuff tears if left untreated over time.
Traumatic shoulder injuries
- Shoulder dislocation — the humeral head slips out of the glenoid, usually anteriorly (forward) after a fall or forceful contact. Young patients who dislocate have a high recurrence rate (up to 80% in patients under 20) and may need surgical stabilization
- Fractures, clavicle (collarbone) fractures are common from falls. Proximal humerus fractures are more common in older adults with osteoporotic bone
- Labral tears (SLAP lesions), tears of the cartilage ring around the socket, often from repetitive throwing or a fall on an outstretched arm. Produce a clicking or catching sensation and deep shoulder pain
- AC joint injuries — damage to the acromioclavicular joint at the top of the shoulder, usually from a direct fall onto the point of the shoulder
When to See an orthopedic shoulder specialist
Get your shoulder evaluated if:
- Pain persists for more than 2–3 weeks despite rest and over-the-counter pain relief
- You're unable to raise your arm to shoulder height or above
- Pain disrupts your sleep, you can't lie on the affected side
- You notice visible swelling, deformity, or bruising around the shoulder
- The shoulder feels unstable, as if it could slip out
- Weakness has developed, you drop objects or can't hold your arm up against mild resistance
- Pain started after a fall, collision, or sudden forceful movement
Delaying evaluation when these signs are present often leads to stiffer joints, weaker muscles, and a longer rehabilitation.
Diagnosis of shoulder pain
Clinical evaluation
A thorough shoulder exam takes 10–15 minutes and gives more diagnostic information than any scan. I'll assess:
- Range of motion — active (you move it) and passive (I move it for you). If active motion is limited but passive motion is full, the problem is likely muscular or tendinous. If both are limited, the capsule or joint itself is involved
- Strength testing, specific tests for each rotator cuff muscle (Jobe's test for supraspinatus, external rotation for infraspinatus/teres minor, belly press for subscapularis)
- Impingement signs, Neer's test, Hawkins-Kennedy test
- Instability tests — apprehension test, load-and-shift test for patients with suspected dislocations
- Palpation, checking for tenderness at the AC joint, biceps tendon groove, and rotator cuff insertion
Imaging tests
- X-rays, first-line imaging. Shows fractures, arthritis, calcific tendinitis, AC joint abnormalities, and bone spur formation
- MRI — the gold standard for soft tissue evaluation. Detects rotator cuff tears (and their size), labral tears, capsular thickening, and bone marrow edema. I order an MRI when clinical examination suggests a structural tear or when symptoms persist despite 6–8 weeks of conservative treatment
- Ultrasound, useful for dynamic assessment of the rotator cuff. I can watch the tendons move in real time and identify partial tears, tendinitis, and bursitis. It's also used for guided injections

An older adult displaying shoulder discomfort often linked to age-related shoulder arthritis or joint degeneration.
Shoulder injury treatment options
Treatment depends on the diagnosis, severity, the patient's age, activity level, and functional demands.
Non-Surgical treatments
Most shoulder conditions, including rotator cuff tendinitis, mild impingement, early frozen shoulder, and mild arthritis — respond to conservative management:
- Activity modification, avoiding the aggravating movement while staying active in non-painful ways. Complete immobilization is rarely advised
- NSAIDs, ibuprofen or naproxen for 1–2 week courses during acute flares
- Physiotherapy — the single most effective non-surgical intervention for most shoulder problems. A structured program typically includes:
- Pendulum exercises (early phase, to maintain motion without loading the joint)
- Passive and active-assisted range of motion exercises
- Rotator cuff strengthening with resistance bands (isometric first, then isotonic)
- Scapular stabilization exercises (wall push-ups, serratus punches, rows)
- Postural correction
- Corticosteroid injections, subacromial injections can provide 4–12 weeks of pain relief, creating a window for physiotherapy to be more effective. I typically limit injections to 2–3 per joint per year. Repeated steroid injections can weaken tendons over time
- Hyaluronic acid injections, occasionally used for shoulder arthritis, though the evidence is stronger for knee arthritis
Surgical treatment options
Surgery is considered when conservative treatment fails after an adequate trial (usually 3–6 months), or in cases where the diagnosis itself warrants early surgical intervention (large acute rotator cuff tears, shoulder dislocations in young athletes, displaced fractures):
- Arthroscopic rotator cuff repair — small incisions, camera-guided repair of the torn tendon back to bone using suture anchors. Recovery involves 4–6 weeks in a sling, followed by graduated physiotherapy over 4–6 months. Full strength recovery typically takes 9–12 months
- Subacromial decompression, arthroscopic removal of bone spurs and inflamed bursa to create more space for the rotator cuff tendons. Often combined with rotator cuff repair
- Arthroscopic capsular release, for refractory frozen shoulder that hasn't responded to physiotherapy and injections. The tight capsule is cut under direct visualization, followed by immediate physiotherapy
- Shoulder stabilization surgery — for recurrent dislocators, the torn labrum is reattached (Bankart repair) or the capsule is tightened to prevent the humeral head from slipping out
- Shoulder replacement, for end-stage arthritis. Total shoulder arthroplasty replaces both the ball and socket. Reverse shoulder arthroplasty (which switches the positions of the ball and socket) is used when the rotator cuff is irreparably torn alongside arthritis. Modern implants and surgical techniques have made shoulder replacement a highly successful procedure with 90–95% patient satisfaction rates
Recovery and rehabilitation
Post-Treatment recovery timelines
- Rotator cuff tendinitis/impingement, 6 to 12 weeks of physiotherapy. Most patients feel significantly better by week 4–6
- Frozen shoulder — 6 months to 2 years for full resolution. Active treatment with physiotherapy and injections can cut this timeline
- Arthroscopic rotator cuff repair, sling for 4–6 weeks, return to desk work in 2–3 weeks, light activities by 3 months, full recovery 6–12 months
- Shoulder replacement, sling for 2–4 weeks, driving by 6 weeks, return to most activities by 3–4 months
Key rehabilitation principles
- Don't push through sharp pain during exercises — a dull stretch is acceptable; a sharp stab is not
- Consistency matters more than intensity. Short daily sessions outperform occasional intense ones
- Avoid heavy lifting and overhead work during the healing period
- Follow your physiotherapy program completely. Stopping early because "it feels better" is one of the most common reasons I see recurrence
Preventing shoulder pain
- Maintain good posture, rounded shoulders and a forward head position narrow the subacromial space and predispose to impingement. If you work at a desk, set up your screen at eye level and take breaks every 45–60 minutes
- Warm up before exercise, 5 minutes of arm circles, cross-body stretches, and band pull-aparts before upper body workouts
- Strengthen the rotator cuff — external rotation with a resistance band (3 sets of 15, three times per week) is one of the simplest and most effective preventive exercises
- Don't ignore early symptoms, mild shoulder discomfort that doesn't resolve in a week deserves attention, not avoidance
- Avoid repetitive overhead work without breaks, painters, electricians, and overhead press enthusiasts all share elevated risk for impingement and rotator cuff problems
If shoulder pain is interfering with your daily activities or isn't settling with rest and simple measures, get it looked at sooner rather than later. At my clinic at KDSG Hospital, Noida, I offer detailed clinical evaluation and imaging-based diagnosis, along with both non-surgical and surgical treatment options tailored to each patient's specific condition, age, and activity goals.
Medical Disclaimer
The information provided on this website is for educational purposes only and should not be considered as medical advice. Please consult Dr. Ankur Singh or a qualified healthcare professional for personalized medical guidance.



























