Hip replacement surgery explained: Who needs It and what to expect

Surgical team conducting advanced orthopedic surgery such as hip replacement.
Hip pain that doesn't respond to medication, physiotherapy, or lifestyle changes can eventually take over your life. Getting out of a chair becomes a task. Walking across a room feels like effort. Sleep gets interrupted because there's no comfortable position. When pain reaches this stage, when it controls what you do and don't do, hip replacement surgery becomes a serious conversation.
I've performed hundreds of hip replacements over 15+ years of orthopedic practice, and I can say this with confidence: for the right patient, at the right time, this surgery is one of the most successful procedures in all of medicine. Patient satisfaction rates exceed 95%. But surgery isn't the starting point. It's the last step after other treatments have been exhausted. Let me walk you through who actually needs it, what happens during and after the procedure, and what recovery looks like in practical terms.
Understanding Hip pain and Hip arthritis
The hip is a ball-and-socket joint — the femoral head (ball) sits inside the acetabulum (socket) of the pelvis. A layer of articular cartilage, typically 3-4 mm thick, covers both surfaces. This cartilage allows smooth, frictionless movement and absorbs impact during walking, running, and climbing.
When this cartilage degrades, through wear, disease, or injury, the protective barrier disappears. Bone grinds against bone. The joint becomes inflamed, stiff, and painful.
Common causes of severe Hip damage
- Osteoarthritis — the most frequent cause. Cartilage wears down gradually over years. Age, genetics, obesity, and prior joint injury all accelerate the process. X-rays show progressive joint space narrowing, osteophyte (bone spur) formation, and sclerosis.
- Rheumatoid arthritis, an autoimmune condition where the body's immune system attacks the joint lining (synovium), causing chronic inflammation and eventual cartilage destruction.
- Avascular necrosis (osteonecrosis), blood supply to the femoral head gets disrupted (from long-term steroid use, excessive alcohol, sickle cell disease, or hip fracture), and the bone tissue dies. The femoral head collapses, destroying the joint surface.
- Hip fractures — especially in elderly patients with osteoporosis. Displaced femoral neck fractures in patients over 60 often require replacement rather than repair because the blood supply to the femoral head is too compromised for the bone to heal.
- Post-traumatic arthritis, previous injuries (fractures, dislocations) that damaged the joint surface, leading to accelerated wear years later.
When Is Hip replacement surgery needed?
Hip replacement is never a first-line treatment. Before recommending surgery, I exhaust conservative options, physiotherapy, weight management, activity modification, anti-inflammatory medications, walking aids, and sometimes corticosteroid or hyaluronic acid injections.
Surgery enters the conversation when these measures fail to provide adequate relief.

Image highlighting back and hip pain commonly associated with joint or muscular problems.
Signs that point toward Hip replacement
- Pain at rest — not just during activity, but while sitting or lying down
- Night pain that regularly disrupts sleep
- Difficulty walking more than a few hundred meters
- Stiffness that limits basic movements like bending to tie shoes or getting in and out of a car
- Failed response to at least 3-6 months of conservative treatment
- X-ray or MRI showing advanced joint damage (bone-on-bone arthritis)
- Significant impact on quality of life, inability to work, socialize, or perform daily tasks
The decision isn't based on a single X-ray finding or a single symptom. It's a clinical judgment that weighs pain severity, functional limitation, imaging findings, patient age, activity level, and overall health. I discuss all of this with my patients before making a recommendation.
Types of Hip replacement surgery
Total Hip replacement (Total Hip arthroplasty)
The most common type. Both the damaged femoral head and the worn acetabulum are replaced with prosthetic components:
- A metal stem inserted into the femur
- A ceramic or metal ball attached to the stem (replacing the femoral head)
- A polyethylene (plastic) or ceramic liner placed inside a metal acetabular cup
Modern bearing surfaces, ceramic-on-ceramic or ceramic-on-polyethylene — are designed to minimize wear. Current implants last 20-25 years in the majority of patients. For patients under 60, ceramic-on-ceramic bearings are often preferred for their superior wear characteristics.
Partial Hip replacement (Hemiarthroplasty)
Only the femoral head is replaced; the natural acetabulum is preserved. This is most commonly performed for displaced femoral neck fractures in elderly patients (typically over 70-75) who have lower activity demands. The surgery is faster, recovery is quicker, but it's not suitable for arthritis, both joint surfaces need to be addressed in that case.
Minimally invasive Hip replacement
Uses smaller incisions (typically 8-10 cm vs. 15-20 cm in traditional approaches) and works between muscles rather than cutting through them. Benefits include less blood loss, less post-operative pain, shorter hospital stay, and faster early rehabilitation. However, it requires specialized training and instrumentation, and isn't suitable for every patient, particularly those with complex anatomy or revision cases.
The anterior approach has gained popularity because it's a true intermuscular approach — no muscles are detached. This allows faster recovery, fewer hip precautions post-surgery, and earlier return to normal activities.
Preparing for Hip replacement surgery
Preparation directly affects surgical outcomes. I take pre-surgical optimization seriously.
Pre-Surgery evaluation
- Complete medical history and physical examination
- Blood tests (hemoglobin, blood sugar, kidney function, coagulation profile)
- X-rays (AP pelvis, lateral hip) and sometimes CT scan for templating
- Cardiac evaluation (ECG, echocardiogram if indicated)
- Pulmonary assessment for patients with respiratory conditions
- Review and adjustment of medications, blood thinners need to be stopped 5-7 days before surgery; diabetic medication may need dosage changes
What patients should Do before surgery
- Strengthen muscles, pre-operative physiotherapy (prehabilitation) for 2-4 weeks improves post-surgical recovery significantly. Stronger quadriceps and gluteal muscles before surgery translate to faster mobilization afterward.
- Optimize weight — excess weight increases surgical risk and slows recovery. Even modest weight loss (3-5 kg) helps.
- Stop smoking, smoking impairs wound healing and increases infection risk. Ideally, stop at least 4 weeks before surgery.
- Arrange home support, you'll need help at home for the first 2-3 weeks. Plan for meal preparation, raised toilet seats, grab bars in the bathroom, and a ground-floor sleeping arrangement if possible.
- Dental clearance — untreated dental infections can seed bacteria to the new joint. Get a dental check-up and treat any active infections before surgery.
What happens during Hip replacement surgery
The procedure typically takes 60-90 minutes under spinal anesthesia (preferred) or general anesthesia.
Surgical steps
- An incision is made (anterior, lateral, or posterior approach depending on surgeon preference and patient factors)
- The damaged femoral head is removed
- The acetabulum is prepared using specialized reamers, and the prosthetic cup is press-fitted or cemented into place
- The femoral canal is prepared with broaches, and the metal stem is inserted
- A trial reduction is performed, the surgeon checks leg length, joint stability, and range of motion
- Final implants are placed and the joint is reduced
- The wound is closed in layers with or without a drain
I use intraoperative fluoroscopy (live X-ray) to verify implant positioning and leg length. This reduces the risk of leg length discrepancy, one of the most common patient concerns after hip replacement.
Recovery after Hip replacement surgery
Recovery follows a predictable timeline, but individual variation exists based on age, fitness level, and surgical approach.
Hospital stay (Days 1-3)
- Most patients stand and take a few steps with a walker within 12-24 hours of surgery
- Pain is managed with a multimodal protocol — nerve blocks, oral analgesics, and ice therapy
- A physiotherapist visits daily for gait training and basic exercises
- Blood clot prevention with medication (typically low-molecular-weight heparin) and compression stockings
- Discharge typically on day 2-3 for uncomplicated cases
Early recovery at home (Weeks 1-6)
- Walking with a walker or crutches for the first 2-3 weeks, then transition to a walking stick
- Physiotherapy 3-5 times per week, focusing on range of motion, quadriceps activation, and gait normalization
- Wound care, keep the incision clean and dry. Staples or sutures are removed at 10-14 days
- Avoid low chairs, crossing legs, and bending past 90 degrees (if posterior approach was used)
- Driving: typically possible by week 4-6 (automatic transmission) once you're off narcotic pain medication and can perform an emergency stop safely
Full recovery (3-6 months)
- Most patients walk without any aid by 6-8 weeks
- Return to desk work: 4-6 weeks. Physical labor: 3-4 months.
- Full bone ingrowth into uncemented implants takes approximately 6-12 weeks
- Low-impact activities (swimming, cycling, walking, golf) are encouraged long-term
- High-impact activities (running, jumping, contact sports) are generally not recommended as they accelerate implant wear
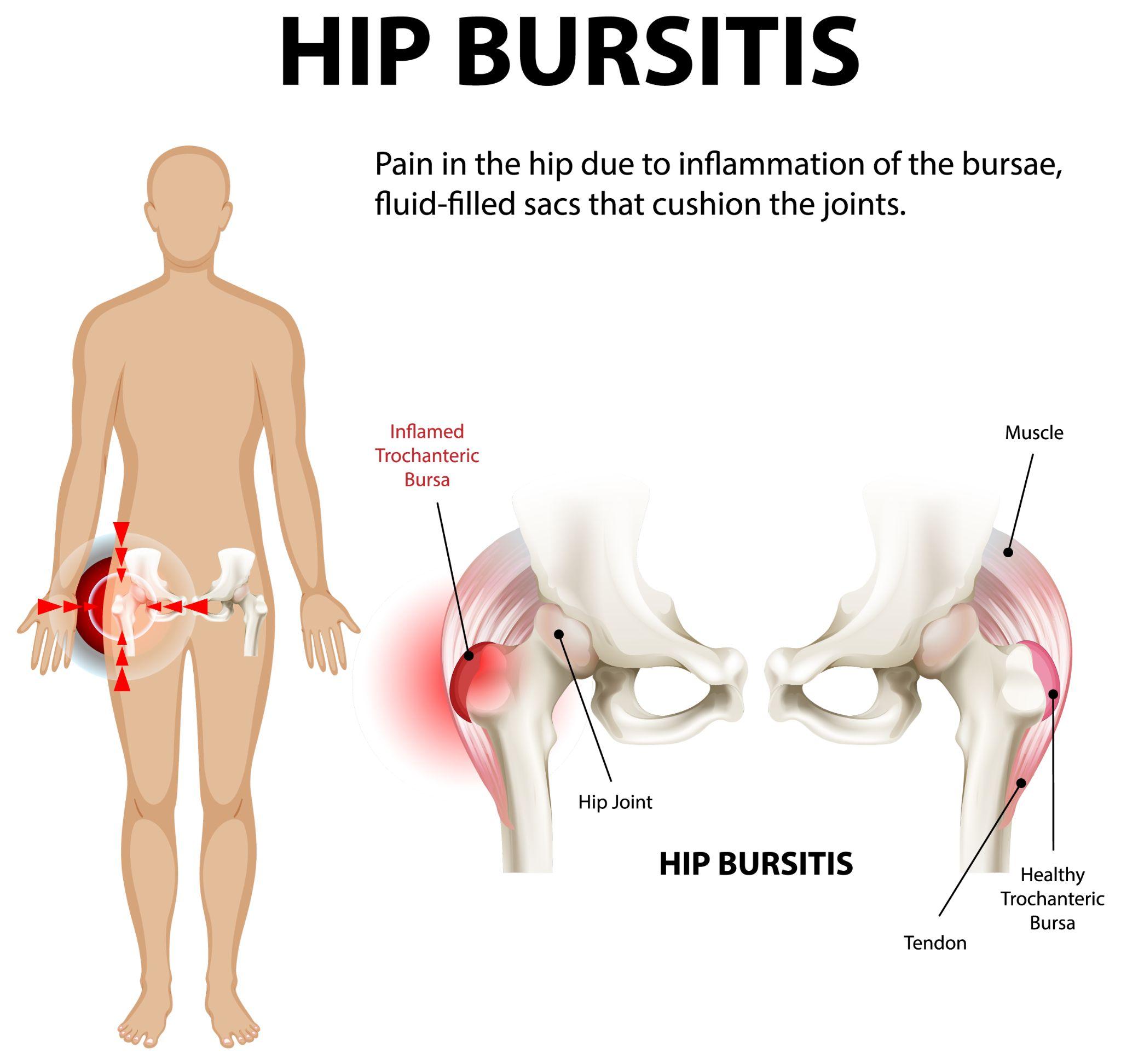
Visual representation of hip bursitis showing inflamed bursae causing hip pain.
Risks and complications
Hip replacement is a safe, well-established procedure, but no surgery is risk-free. Potential complications include:
- Infection (1-2% risk) — minimized through prophylactic antibiotics, sterile technique, and laminar airflow operating theatres
- Blood clots (DVT/PE), prevented with early mobilization and anticoagulant medication
- Implant dislocation (2-3% with posterior approach, <1% with anterior approach), reduced by following post-operative precautions
- Leg length discrepancy — careful intraoperative measurement and templating minimize this risk
- Implant loosening, rare in the first 15-20 years with modern implants; more common in younger, more active patients
- Nerve injury, uncommon (<1%) but can cause temporary numbness or foot drop
Choosing an experienced surgeon who performs a high volume of hip replacements reduces complication rates measurably.
Life after Hip replacement
Most patients describe hip replacement as life-changing. The constant pain that defined their days — gone. The stiffness that made every movement a negotiation, resolved. Activities they'd given up, walking in a park, playing with grandchildren, traveling — become possible again.
Modern implants are designed for durability. With reasonable activity levels and regular follow-up (I recommend X-rays at 1 year, 5 years, and every 5 years thereafter), most implants will outlast the patient.
The difference comes down to timing and expertise. Waiting too long allows muscles to weaken, gait patterns to deteriorate, and the opposite hip or knee to develop compensatory problems. Getting assessed at the right time, and by the right surgeon, determines your outcome.
Dr. Ankur Singh provides individualized orthopedic care with a focus on precise diagnosis, advanced surgical techniques, and structured rehabilitation. For patients considering hip replacement, a thorough evaluation helps clarify whether surgery is needed now, can be delayed, or can be avoided altogether.
Medical Disclaimer
The information provided on this website is for educational purposes only and should not be considered as medical advice. Please consult Dr. Ankur Singh or a qualified healthcare professional for personalized medical guidance.



































